The management of a gummy smile without surgery, about a case report
The most attractive smile according to Tunisian orthodontists, dentists and laypersons
15 février 2021Réussir une Prothèse implanto-portée dans le secteur antérieur : A propos d’un cas clinique
22 mars 2021Rim Ben Elkahla*, Mounira Rtibi*, Pr Anissa Elyemni Zinelabidine**, Pr Abdelatif Boughzala**
* orthodontic residents in Farhat Hached Hospital-Sousse Tunisia
** orthodontic professors in Farhat Hached Hospital-Sousse Tunisia
E-mail: rimbenelkahla@gmail.com
Abstract
A perfect smile is dictated by the balance among 3 parameters: the white (teeth), the pink (gum), and the lips: excessive gingival display while smiling has been a cause of esthetic embarrassment for many patients and is one of the most common complaints of them seeking an aesthetic smile, thus affecting their psychosocial behavior. There are various alternatives for correcting a gingival smile, ranging from techniques such as gingivectomy to more complex and invasive procedures such as orthognathic surgery.
This case report describes the treatment of a skeletal Class I malocclusion with a convex profile, involving a gummy smile. The maxillary incisors were intruded with super chain anchored to a mini-implant.
The aim of present case report is to discuss an alternative to orthognathic surgery “correction of deep overbite and gummy smile by using a mini-implant”.
Keywords
gummy smile / miniscrews / surgery / intrusion
Introduction
Smiling involves criteria of beauty to which society today gives increasing importance and, while the smile may be a ‘‘killer app’’ for some people, it can constitute a real complex, or indeed a handicap, for others, especially in some forms of ‘‘gummy smile’’[16].
Excessive gingival display during smiling, or gummy smile, is an aesthetic problem for some patients [1-4]. It may result from a variety of etiological factors [5-6]; therefore, proper diagnosis is critical before beginning the treatment [5,6]. In adults, when the gummy smile is caused by overgrowth of anterior vertical maxillary excess, the outcome may not always be successful by conventional orthodontic therapy alone. In such cases, surgical therapy, such as Le Fort impaction is often indicated to achieve a good smile [1,3,7-9]. However, if patients are unwilling to undergo surgical treatment, an alternative method must be considered to treat the gummy smile. The traditional therapies, such as high-pull headgear [10,11], may not work properly in adults. Some investigators have shown successful intrusion of teeth with mini-implants as anchorage and maxillary gingivectomies [4,10]. Lin et al. [6] demonstrated successful treatment of gummy smile patients using that skeletal anchorage. The present clinical case describes the treatment of an adult patient with gummy smile using miniscrew anchorage, maxillary gingivectomies and lip repositioning [4].
Diagnosis and etiology
A healthy 25-year-old Tunisian female patient presented to our Orthodontic Department in Farhat Hached Hospital with the chief complaint of gummy smile.
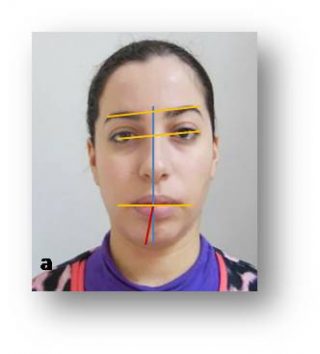
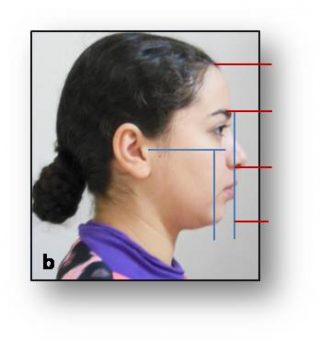
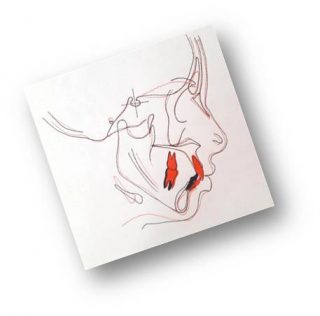
Facial examination (Fig1) showed a chin deviation from the mid-sagittal plane toward the right side, convex profile. She showed excessive gingival display of 5 mm in both the anterior and posterior areas upon smiling.
Side view: Ortho frontal profile, harmonious with an equality of the floors of the face.
Study of the smile: the gingival smile is the result of the association of several etiologies which are important contraction of the levator upper lip muscle, Excess of attached gum and Supraalveolia + Supraclusia, Premolar endoalveolia without lateral inversion (corridors oral).
 |
 |
 |
 |
|---|---|---|---|
| Fig. 1: Pre-treatment facial photographs. | |||
| a. Facial view | b. Lateral view | c. Smile view | d. gymmy smile assessment |
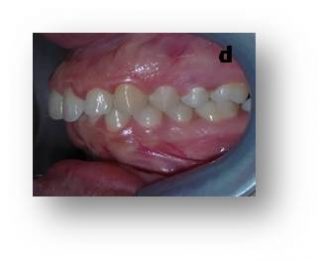
The intraoral examination (Fig 2) revealed Class I molar relationship on the left side and one-half unit Class II relationship on the right side, little mandibular arch crowding, 4-mm overjet, and deep over bite, and the maxillary midline was deviated 3 mm to the left.
 |
||
 |
 |
 |
 |
||
|
Fig.2: intraoral photographs a.maxillary arch b. right side c. anterior occlusion d. left side e. mandibular arch |
||
The radiological evaluation revealed:
The panoramic (fig3) showed a rounded Right condyle, a thick left condyle, Right ramus shorter and thicker than that on the left side.
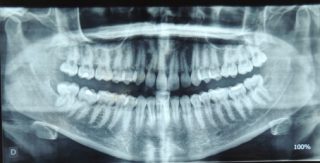
Fig.3: pretreatment panoramic |
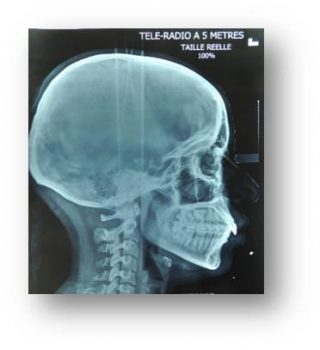
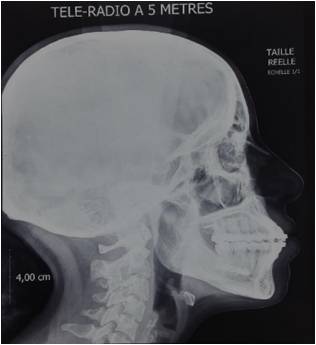
The cephalometric analysis (table 1) using lateral teleradiography (fig4) showed a skeletal Class I relationship (ANB =3°). The frontal teleradiography (fig5) revealed a mandibular laterognathia.
 |
 |
|
Fig.4: pretreatment lateral teleradiography |
Fig.5: pretreatment frontal teleradiography |
| Cephalometric measurements | Pre-treatment | Post-treatment | Norms |
| SNA | 76° | 76° | 82°+- 2 |
| SNB | 73° | 75° | 80 +-2 |
| ANB | +3° | 1° | 2°+- 2 |
| AoBo | 0mm | -3mm | 0mm+- 2 |
| FMIA | 56° | 50° | 68° |
| IMPA | 92° | 95° | 87° |
| FMA | 32° | 30° | 22°-28° |
| GoGn/SN | 30° | 30° | 32° +- 5° |
| I/i | 125° | 123° | 135° |
| I/F | 110° | 112° | 107°+-5 |
| Z | 55° | 59° | 78° |
| Table.1: cephalometric summary | |||
Treatment objectives
- Reduce the gummy smile
- Correct the maxillary midline and obtain a good functional Class I molar and canine relationship
- Restore a functional overjet and overbite;
- Correction of the shape of the arches
- Correction of mandibular asymmetry
TREATMENT ALTERNATIVES
This patient showed excessive gingival display in both the anterior and posterior areas with a large difference in the gingival heights between the maxillary anterior and posterior teeth. To correct the gummy smile, therefore, we decided to intrude the entire upper dentition instead of focusing only on the upper anterior teeth. Two treatment options were discussed with the patient. The first was traditional orthodontic treatment combined with Le Fort I surgery to reduce the maxillary height, which would, in turn, reduce the gingival exposure. The second option was orthodontic intrusion of the entire maxillary dentition using miniscrew skeletal anchorage. After a review of the risks and benefits of the two options, the patient chose the latter more conservative method.
Treatment plane/progress:
An orthodontic-surgical treatment without extraction was chosen:
After leveling the denture, intrusion of the entire maxillary dentition using 4 miniscrews in order to improve the patient’s smile as much as possible (reduce the ENA/I alveolar component).
Thus, depending on the type of movement desired, the mini screws are positioned in different ways:
two minivis placed in mesial of the canines when one wishes the ingression of the six anterior teeth while controlling the axis of the canines.
the intrusion of the posterior teeth is one of the most difficult movements to carry out, in case of gingival smile, one makes a parallel intrusion, an intrusion of the molars as well as the premolars by positioning a minivis between the 6 and the 7 on each side.
the traction is made with super chains which are changed every two weeks
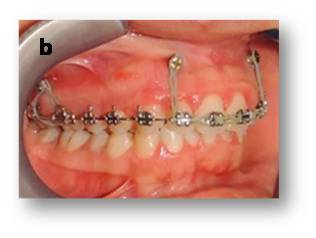
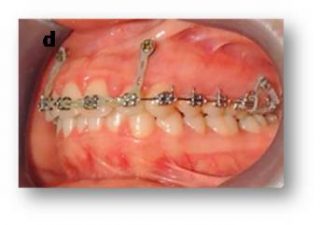
Maxillary first molars were banded transpalatal arch to counteract buccal crown tipping toward the mini-implants. (fig6, fig7)
 |
||
 |
 |
 |
|
Fig.6: intrusion of the entire maxillary dentition using 4 miniscrews a.maxillary arch b. right side c. anterior occlusion d. left side |
||
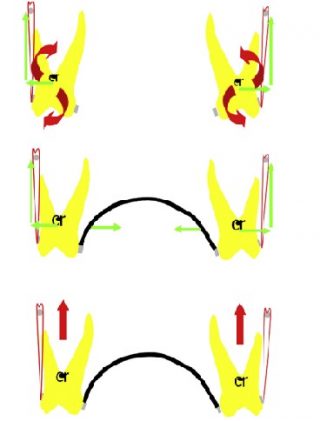
Fig.7: Maxillary first molars banded by transpalatal arch |
 |
 |
 |
| Fig.8: Results after maxillary intrusion | ||
A lip repositioning and gingivectomy were indicated to restore correct gingival morphology, removing a strip of outlined mucosa by a superficial split thickness dissection, leaving the connective tissue exposed. this procedure obtains 80% average reduction in gingival display and prevent the significant elevation of the upper lip when smiling.
 
Fig.9: Result after labial repositioning surgery and gingivectomy |
The patient underwent Obwegezer mandibular derotation surgery for the correction of mandibular laterognathy. the sagittal osteotomy can consist in advancing, moving backwards or correcting the asymmetry of the mandible.
 
Fig.10: Result after the derotation of the mandible by the Obwegeser surgery |
Treatment results
This specific case clearly showed satisfactory esthetic results, the gummy smile was eliminated, and in full smile view, the patient showed no more than 1 to 2 mm of gingiva. The post-treatment photographs demonstrated Class I canine and molar relationships with normal over bite and overjet, and the dental midlines were coincident to each other and with the facial midline (Fig. 11 and 12).
The cephalometric analysis (Table 1) and superimposition (fig13,14,15,16) showed intrusion of maxillary incisors and molars, and the derotation of the mandible by the Obwegeser surgery and a significant improvement in teeth inclinations and angulations.
 |
 |
 |
| Fig. 11: (a,b,c) External photographs and (e) smile at end of treatment | ||
 |
||
 |
 |
 |
 |
||
|
Fig. 12: Post-treatment intraoral photographs. a.Maxillary arch b. right side c. anterior occlusion d. left side e. Mandibular arch |
||
 |
 |
| Fig.13 :Posttreatment panoramic | Fig.14: Posttreatment lateral teleradiography |
 |
 |
 |
| Fig.15 : general super–imposition |
Fig.16: local super-imposition a.Maxilla b. Mandible |
|
Discussion
The reasons for a gummy smile include excessive maxillary vertical growth, over-eruption of the maxillary incisors, incomplete anatomic crown exposure, hyperactivity of the elevator muscles of the upper lip, or a combination of these factors [12].
A gummy smile of skeletal origin requires orthognathic surgery for correction. Dentoalveolar gummy smiles caused by overeruption of the maxillary incisors can be corrected by intruding the extruded maxillary incisors.
The dentogingival type of gummy smile is related to abnormal dental eruption or lack of gingival recession and requires lengthening of the anatomic crown. The neuromuscular type of gummy smile is caused by hypercontractibility or excessive muscle contraction and can be improved by Labial repositioning.
Therefore, proper diagnosis is critical before beginning the treatment.
For this patient, the gummy smile seemed to be a result of hyperfunctional upper lip elevator muscles, excess of attached gingiva and overbite. It was improved using an orthodontic approach mimicking Le Fort I maxillary impaction surgery, lip reposition and gingivoplasty.
The development of mini-screw bone anchorage has extended the possibilities of orthodontic treatment: anterior vertical excess found in adults can now be corrected by intrusion, limiting unwanted side effects in the posterior sectors by appropriate mini-screw positioning.
In this case report, we treated a skeletal class I malocclusion with mandibular laterognathia, and a gummy smile using miniscrews, which were placed in the upper posterior and anterior areas. Maxillary first molars were banded with transpalatal arch(fig6,7) to control the tendency of maxillary teeth to incline in the buccal direction due to the force of super chain from the mini-implants, the transpalatal arch was also adjusted to allow posterior movement of the left teeth.
This case report demonstrated that the use of miniscrew anchorage for maxillary intrusion associated with lip repositioning and gingivectomy is a viable alternative to orthognathic surgery for some patients who present with the chief of complain gummy smile and reject surgical treatment.
Indeed, skeletal anchorage has revolutionized orthodontic anchorage by making it perfectly stable and providing results beyond the realms of conventional orthodontic treatment. [17]
More recently, type A botulinum toxin injection, essentially described by Polo in 2005, has provided a nonoperative solution. Reduced exposure is obtained by weakening upper-levator muscle contractility. This is reversible, and injection has to be renewed. [16]
Conclusion
Each patient should be individually evaluated to determine if a nonsurgical approach may provide acceptable correction. The orthodontic treatment with skeletal anchorage cannot replace orthognathic surgery; however, considering the costs and risks of surgery, it may be used as an alternative for selected cases and if a patient refuses surgery, as demonstrated in this successful case of correction of gummy smile.
References
1. Kokich VG. Esthetics: the orthodontic-periodontic restorative connection. Semin Orthod 1996;2:21e30.
2. Kokich VG. Esthetics and vertical tooth position: orthodontic possibilities. Compend Contin Educ Dent 1997;18:1225e31.
3. Panossian AJ, Block MS. Evaluation of the smile: facial and dental considerations. J Oral Maxillofac Surg 2010;68:547e54. [4] Kaku M, Kojima S, Sumi H, et al. Gummy smile and facial profile correction using miniscrew anchorage. Angle Orthod 2012;82:170e7.
5. Ackerman MB, Ackerman JL. Smile analysis and design in the digital era. J Clin Orthod 2002;36:221e36.
6. Lin JC, Yeh CL, Liou EJ, Bowman SJ. Treatment of skeletal-origin gummy smiles with miniscrew anchorage. J Clin Orthod 2008;42:285e96.
7. Sarver DM, Weissman SM. Long-term soft tissue response to LeFort I maxillary superior repositioning. Angle Orthod 1991;61:267e76.
8. Capelozza Filho L, Cardoso MA, Reis SABR, Mazzottini R. Surgical-orthodontic correction of long-face syndrome. J Clin Orthod 2006;40:323e32.
9. Pinho T, Figueiredo A. Orthodontic-orthognathic surgical treatment in a patient with Class II subdivision malocclusion: occlusal plane alteration. Am J Orthod Dentofacial Orthop 2011;140:703e12.
10. Umemori M, Sugawara J, Mitani H, Nagasaka H, Kawamura H. Skeletal anchorage system for open-bite correction. Am J Orthod Dentofacial Orthop 1999;115:166e74
11. Paik CH, Woo YJ, Boyd RL. Treatment of an adult patient with vertical maxillary excess using miniscrew fixation. J Clin Orthod 2003;37:423e8.
12. Robbins JW. Differential diagnosis and treatment of excess gingival display. Pract Periodontics Aesthet Dent 1999;11:265-72.
13. Garcia R. Le point sur les protocoles chirurgico-orthodontiques. Actual Odontostomatol 1994;187:447-485.
14. L. Massif , L. Frapier utilisation clinique des minivis en orthodontie.[23-492-A-17] – Doi : 10.1016/S1283-0860(06)45784-5
15. Upadhyay M, Yadav S, Patil S. Mini-implant anchorage for en-masse retraction of maxillary anterior teeth: a clinical cephalometric study. Am J Orthod Dentofacial Orthop 2008;134(6):803-810.
16. E. Izraelewicz-Djebali1,2, C. Chabre1 Gummy smile: orthodontic or surgical treatment?,3J Dentofacial Anom Orthod 2015;18:102 DOI: 10.1051/odfen/2014036
17. Upadhyay M, Yadav S Mini-implant for intrusion: Is it always justified?American journal of orthodontics and dentofacial orthopedics: official publication of the American Association of Orthodontists, its constituent societies, and the American Board of Orthodontics 131(3):298; author reply 298-300DOI: 10.1016/j.ajodo.2007.01.008